
A Steerable Biomedical World Model
For N-of-1 longevity medicine — finding steerable points in complex networks. The physician sets the direction; the model navigates.
For N-of-1 longevity medicine — finding steerable points in complex networks. The physician sets the direction; the model navigates.
Act I · The Problem
Aging involves 12 hallmarks, 20,000 genes, and countless interactions. Traditional single-dimensional models can no longer handle this networked complexity.
Multimorbidity among adults aged 65+ reaches 42.4%. The one-disease-one-model paradigm has failed. 20,000+ genes × 12 Hallmarks × infinite interactions demand a unified framework.
Longevity interventions are inherently N-of-1 trials — every aging trajectory is unique. How do we reason from individual observations to causal mechanisms?
Intervene on one target — how does the system respond? Counterfactual reasoning: choose plan A over B, where does the system go?
42.4%
Multimorbidity rate, age 65+
20,000+
Genes × 12 Hallmarks
656
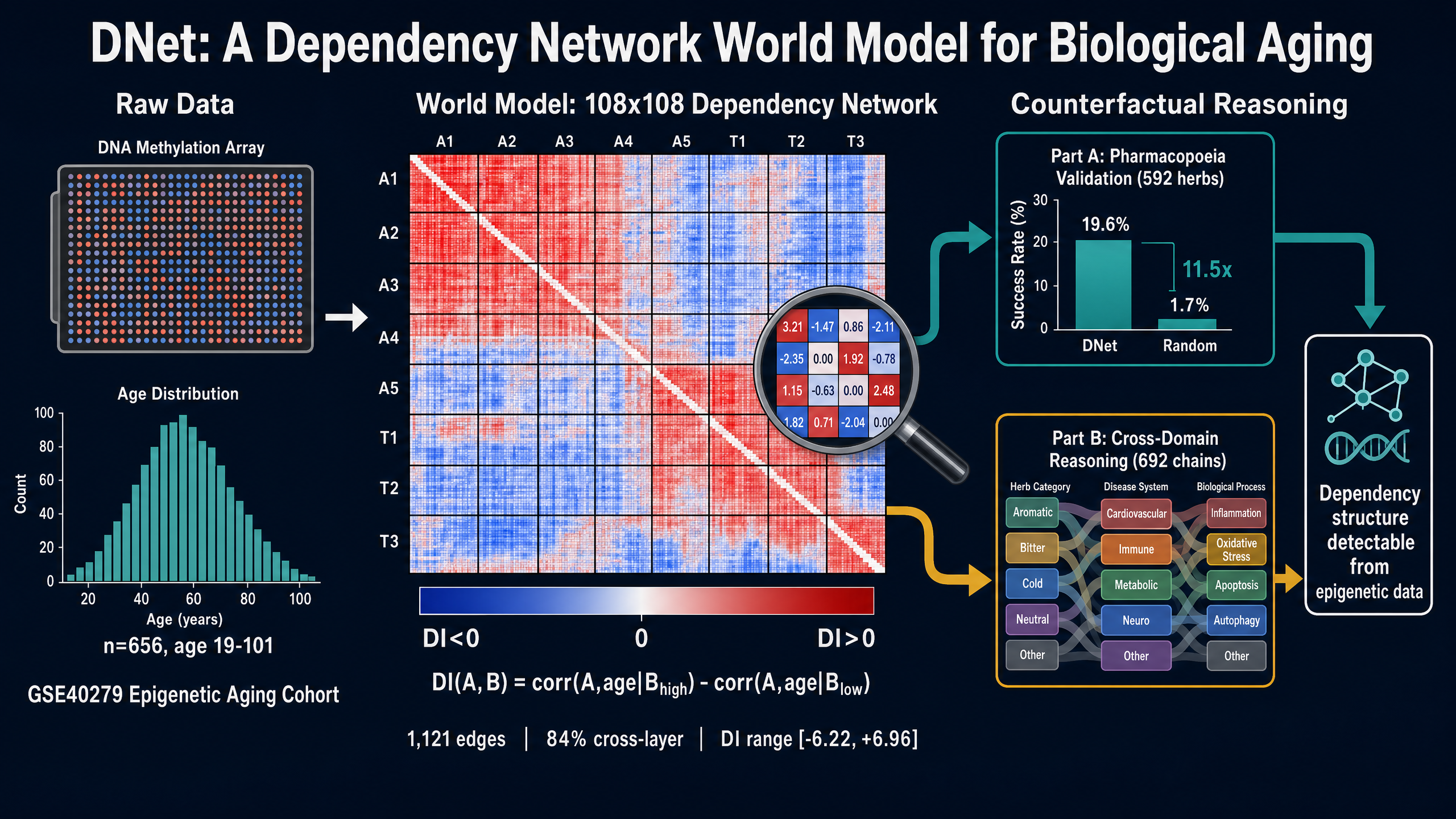
Aging cohort samples (GSE40279)
Two Routes
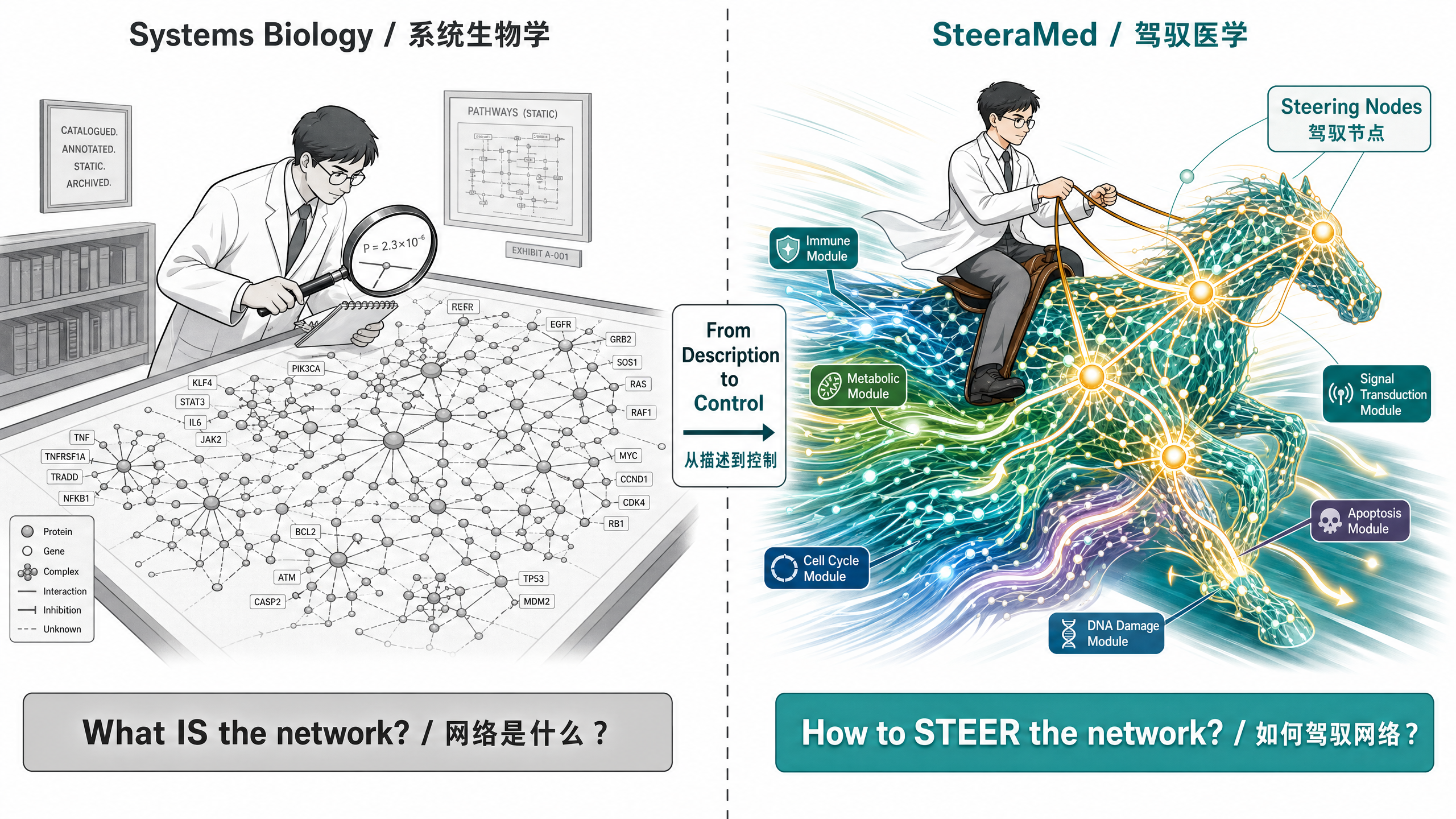
Tries to understand every gear, every pathway, every interaction. The information load is too large for real-time decisions.
You don't need to understand every gear, but you need to know which steering wheel to turn. Finding high-leverage steering nodes in complex networks.
You don't need to understand every gear, but you need to know which steering wheel to turn.
Act II · The Framework
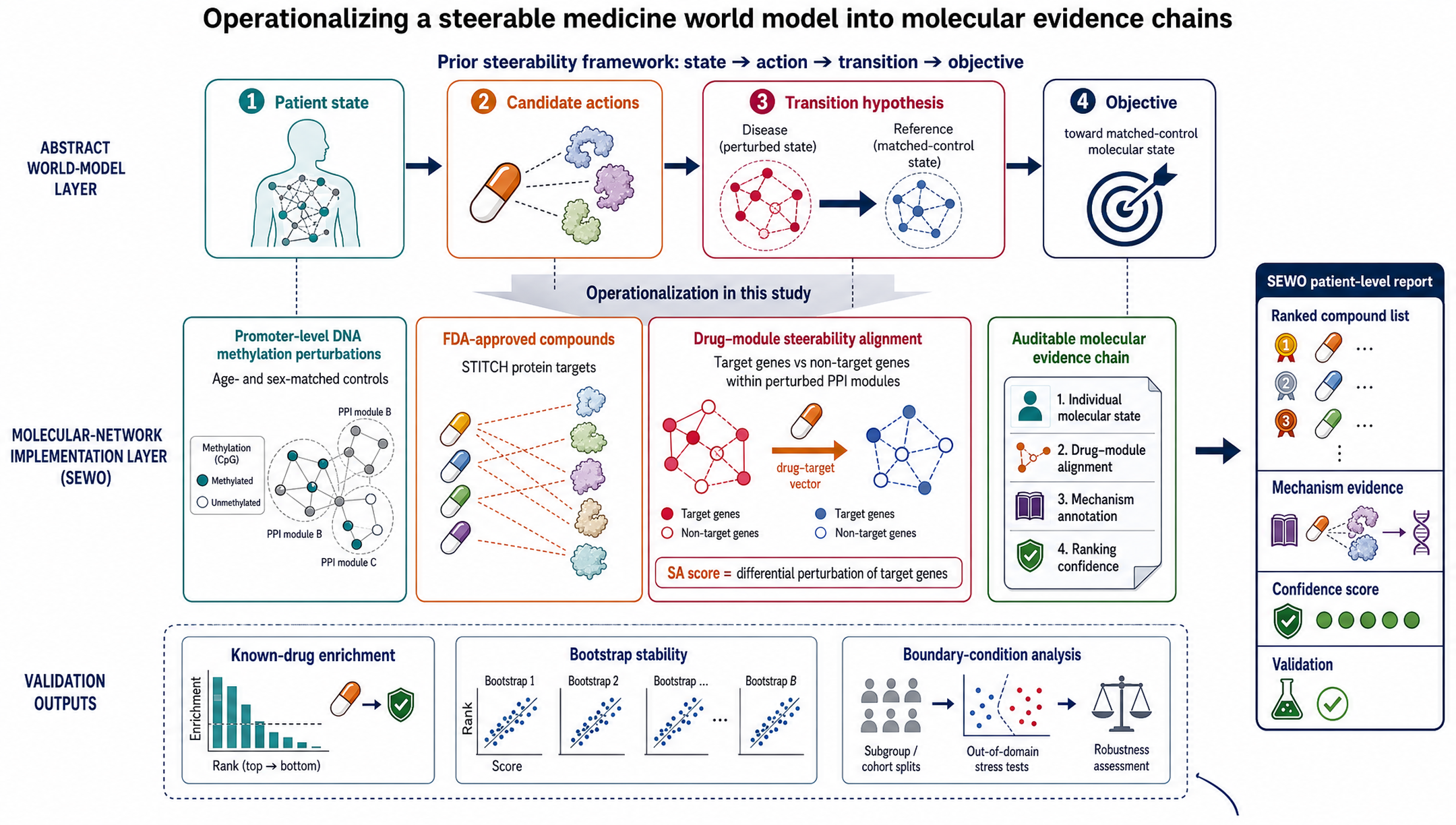
A world model for N-of-1 longevity medicine requires four core capabilities: state perception, intervention-mechanism linkage, response prediction, and individualized recommendation.
DNA methylation reads individual molecular state, quantifying deviation from healthy controls.
DNet dependency network (cross-system state transition rules) + PPI network (drug-target bridge) + compound-target library (action space).
High-leverage nodes in the network: intervening on them drives the largest state transition at the lowest cost.
Δ_i = x_i − x̄_c
where x_i is the individual gene value and x̄_c is the healthy control mean. Each person's deviation pattern is unique — this is the starting point for N-of-1 individualization.
Act III · Dependency Network
108 medical terms, 1,121 dependency edges, bridging Western aging hallmarks and TCM terminology.
85%
Pharmacopoeia efficacy co-occurrence pairs covered by DNet (51/60)
108
Cross-medical-system terminology nodes
7/14
Aging hallmarks whose top-1 TCM consequence is Kidney
DI measures statistical dependency, not causality. In N-of-1 longevity medicine, being actionable matters more than theoretical perfection.
Act IV · PPI Validation
Drug screening tested on four real disease datasets: RA, breast cancer, depression, and aging. The PPI network is a natural bridge between disease mechanisms and drug targets.
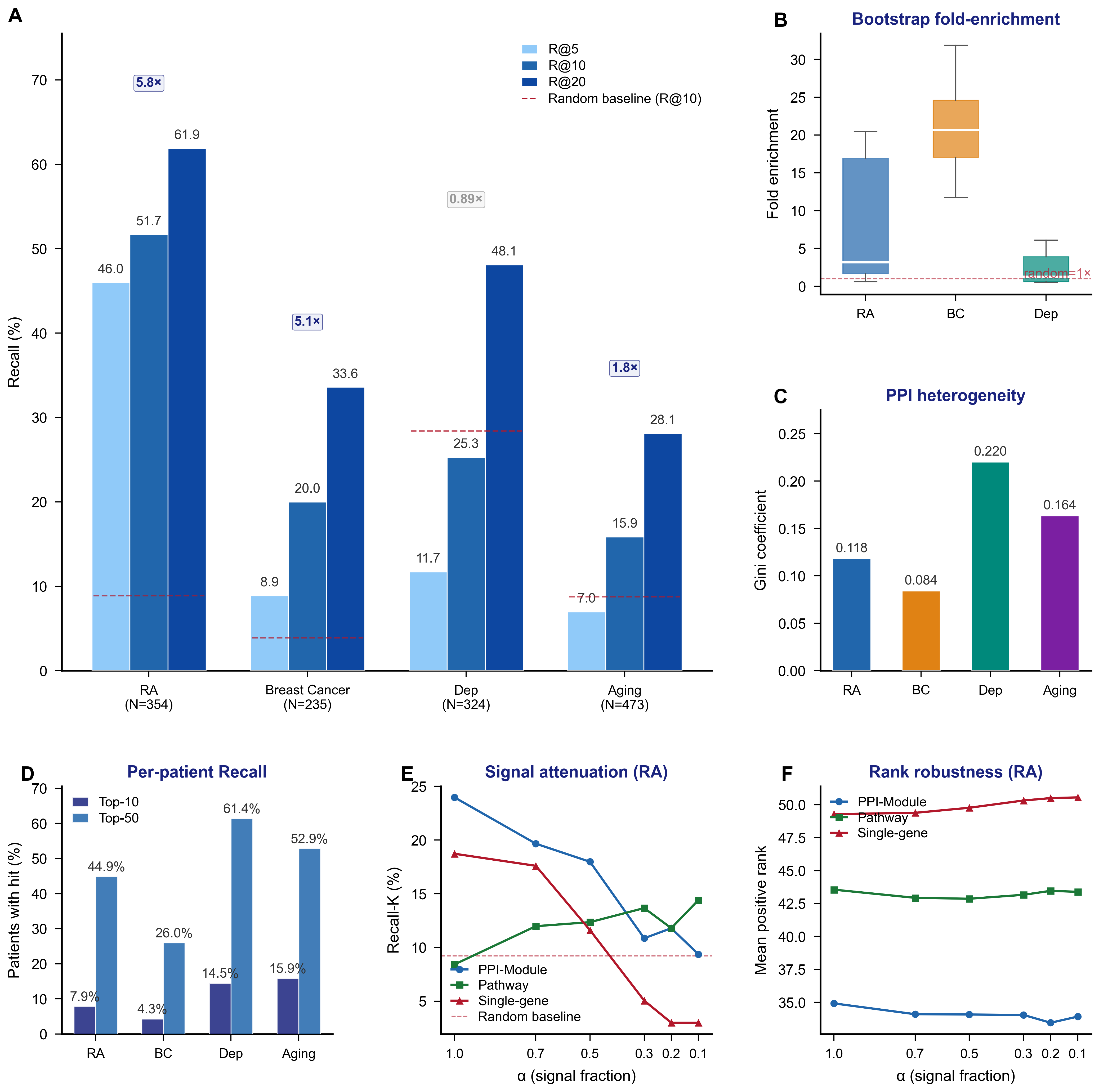
51.7%
5.8× random baseline
Gini 0.20
Depression PPI landscape is robust, creatine top-1 hit rate 6.8%
PPI module-level aggregation outperforms single-gene and pathway methods under noise.
Evidence Chain
A complete reasoning pipeline from individual state to confidence — N-of-1 individualized evidence chains can recapitulate known pharmacology.
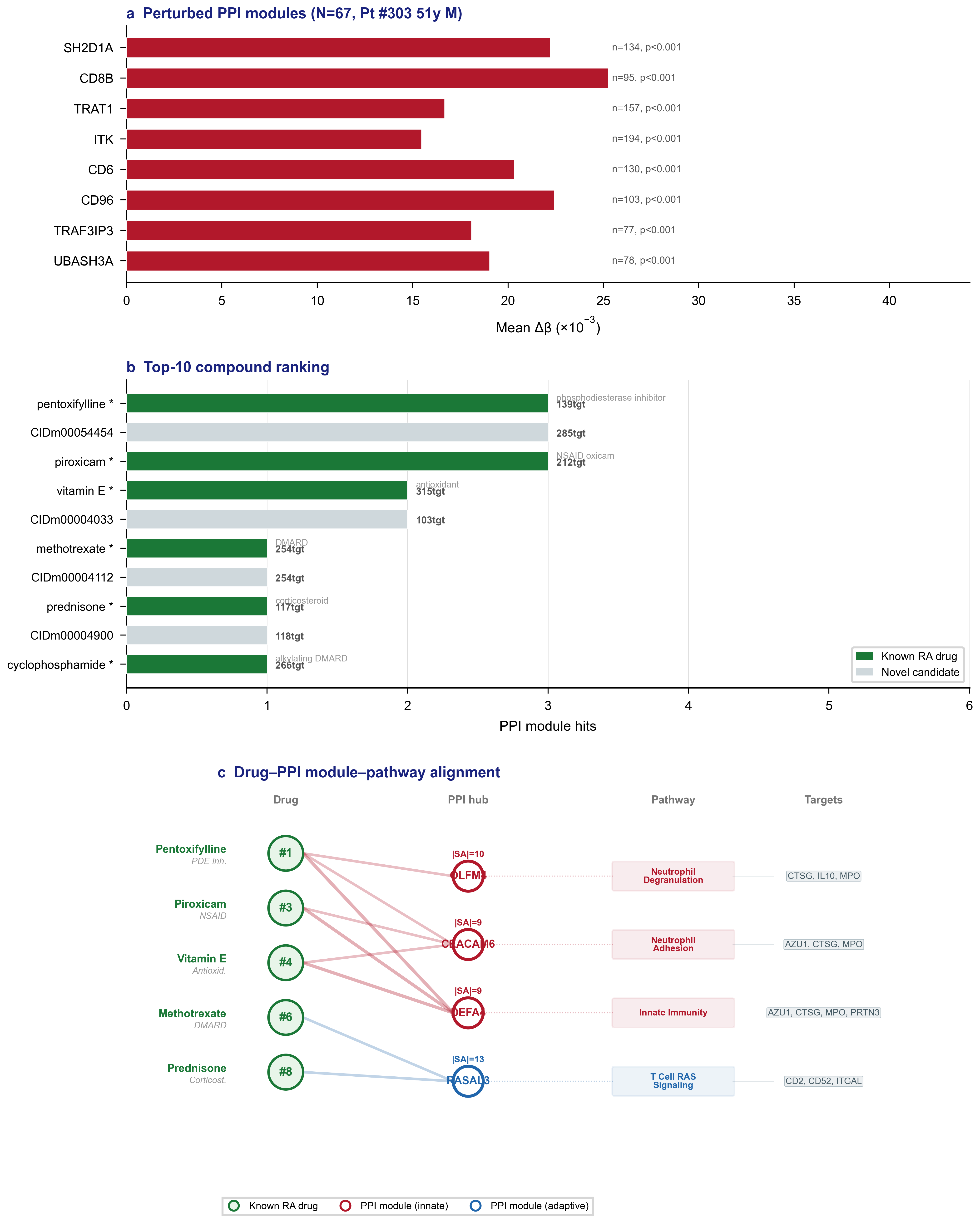
Methylation-perturbed PPI modules (e.g., T-cell: SH2D1A, CD8B)
Compound-target network proximity (Top-10 contains 6 known RA drugs)
Target strength |SA| (CTSG/IL10/MPO, |SA|=9.0-10.2)
Bootstrap stability (200 resamples, imatinib stable at 15%)
Clinical Communication
An aging intervention case — translating the four-layer evidence chain into a patient-friendly three-panel view.
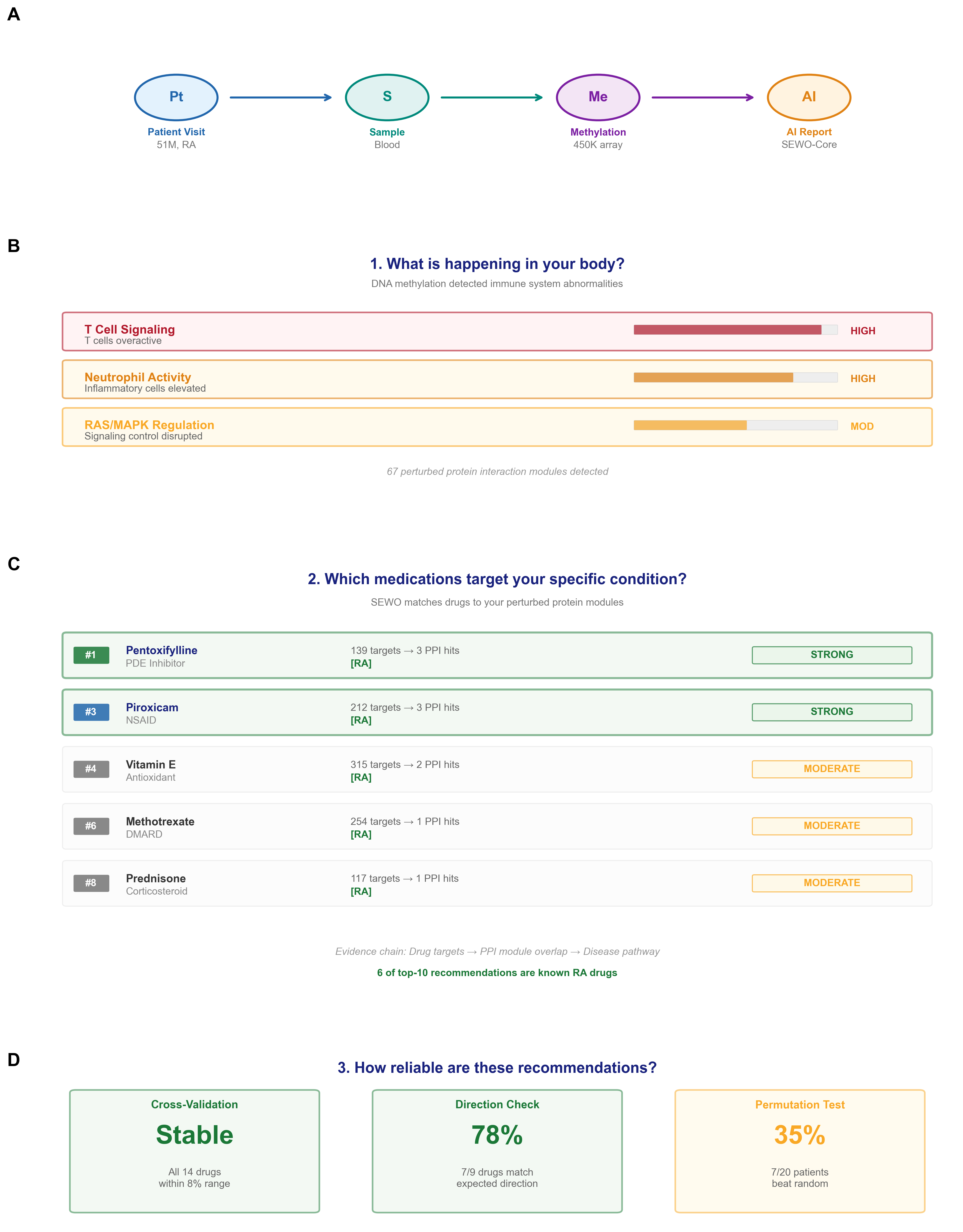
Inflammaging (35 PPI modules) + epigenetic alterations + impaired autophagy
Niacin #1 (30.4% vote share) + Colchicine #2 (29.0%), both literature-convergent candidates
Recall-10=15.9% (1.8× baseline), tier EXPLORATORY
Act V · Roadmap
A four-stage roadmap — from molecular state readout to prospective individualized recommendation.
Current stage: DNA methylation reads individual state, building intervention-mechanism evidence chains.
Near-term: Validate target-binding experimental data for recommended compounds.
Mid-term: N≥500 intervention-response tracking, clinical effect-size validation.
Long-term: Prospective personalized nutrition prescriptions, steerability-prediction accuracy validation.
Conclusion
SteeraMed encodes aging-disease-intervention as a computable network model. The DI index quantifies dependency strength; the steerability metric predicts intervention response.
Predictive power is limited by the scarcity of longitudinal intervention data. More pre-post intervention paired data is needed for calibration. The thickness of the data substrate determines reasoning precision.
Gene-network mapping upgrades TCM experience from fuzzy description to quantifiable network-perturbation models. Modern medicine, TCM, and nutrition science are unified within a single data substrate for the first time.
SteeraMed: A Biomedical World Model for N-of-1 Intervention Reasoning across Chronic Diseases and Aging
DOI: 10.20944/preprints202605.1578.v1
Upload DNA methylation data to obtain a Hallmark-based biological-age assessment and individualized intervention plan.